

On Rapid Tests
On Rapid Tests
Like the first part of my Covid citations, this issue of And Another Thing is free for all Letters readers. Also, it was kind of glitchy on the settings front, so if you got more than one version of this email, I apologize!
Those of you who’ve been following my Pandemic Thoughts for the past year have probably heard me complaining about testing policies as alternatives for vaccination policies, which means it may have seemed like a dramatic shift when, a week or so ago, I posted this:

Because it’s true! Testing alone is inadequate, especially when done infrequently and with a gap of time between test and event. You simply can’t take the information from a PCR test done on Monday and use it to determine if it’s safe to gather with a group on Friday. That’s not how this works, and we’ve known that since very early on.
But I have come around to the idea of day-of rapid screening as a means of providing an extra layer of protection on top of vaccine compliance against the spread of infection, and here’s why:
Our rapid screening tests are less effective than PCR at telling us if we’re infected, but they are very effective at telling us if we’re currently infectious.
This is because rapid antigen screening doesn’t necessarily tell us if we have any Covid in our systems. They have a threshold viral load before they’ll detect the virus in the test sample. But what we know is that the viral load threshold they can detect is a transmissible viral load. That means that if we have crossed the viral load threshold that can be detected by rapid screening, we’re probably contagious, and if we haven’t crossed that threshold, we probably aren’t. And because currently infectious is sometimes a more important piece of information than whether you have any virus in your body at all, it’s a useful tool for us to make day-to-day decisions about things like dinner parties and holiday gatherings.
Michael Mina, an epidemiologist, immunologist, and physician at Harvard Public Health/Medical School adapted the data collected by the UK’s Lateral Flow Oversight Team to this chart showing each of their tests’ sensitivity at detecting contagious viral loads:
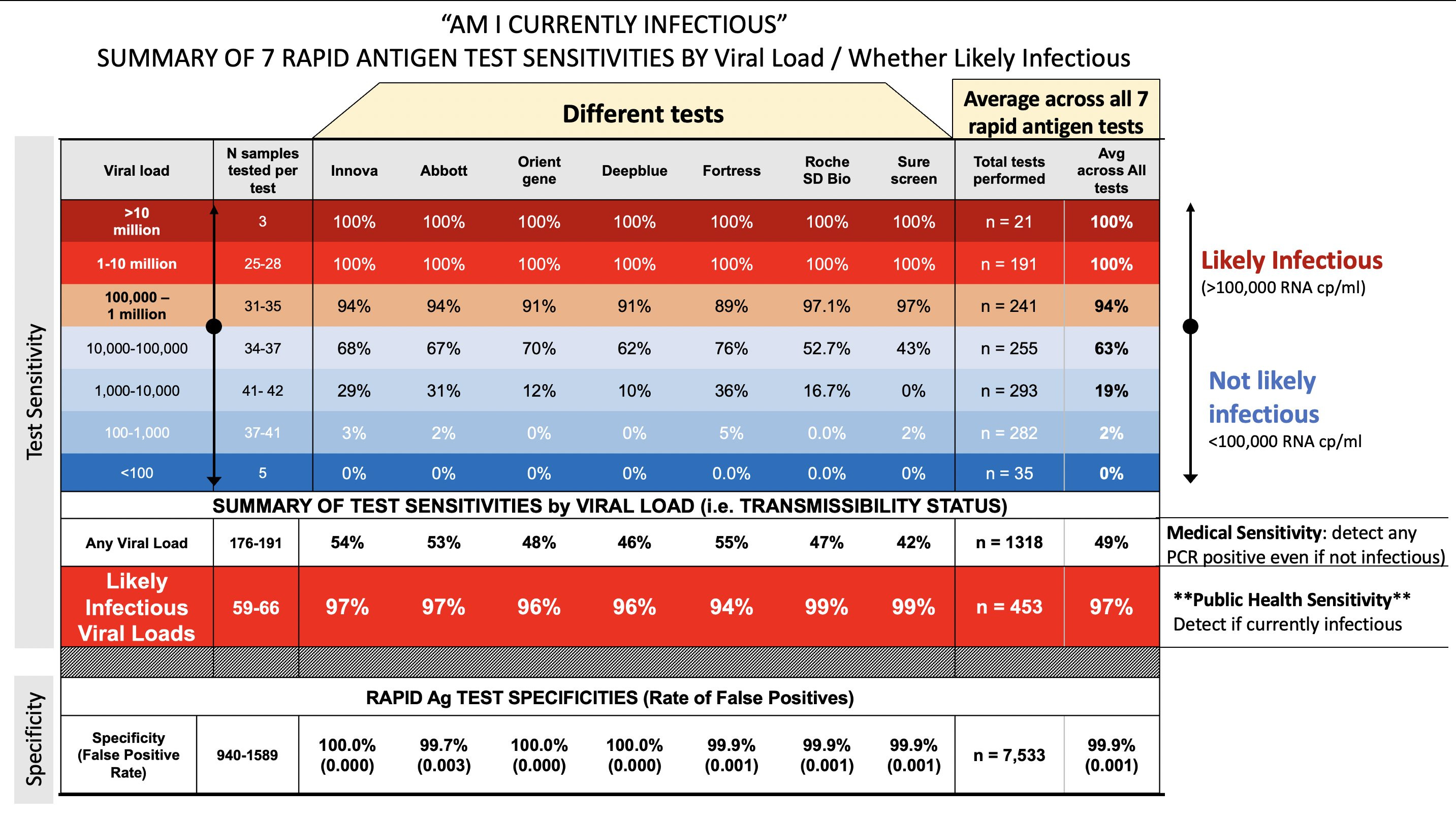
The chart is summarized in a thread on Twitter, in which Mina says that the issue we have is that we’ve been considering rapid tests as medical devices, which means we’re always comparing them to PCR. As medical devices, rapid tests aren’t going to measure up to PCR, because the point of a PCR test is to find out whether you have any Covid at all. PCR tests are much better than rapid tests at detecting trace viral loads as well as post-infectious viral loads. The study’s researchers, in the discussion section of the article, say the same. But what I’m arguing here is that any virus at all isn’t a useful metric for making daily decisions, because that’s not the metric that determines whether we’re going to contract or spread the virus. By shifting our focus to treat rapid tests as public health devices, we can consider their efficacy and sensitivity in their own right and start utilizing them in that way.
The current trend in North America is to skip over rapid testing in favour of the more sensitive PCR, and in Ontario, where I live, they’ve very strictly limited home use of rapid antigen tests because despite successful programs in countries like the UK, Ontario says they can’t trust individuals to perform or report the test correctly. There is legitimate debate about this measure among experts, some of whom argue that accessible home testing will encourage people to abandon other protective measures, or that people will under-report positive tests and fail to seek appropriate verification and care. And those things are probably true, for some people. It’s not a fail-proof measure and can’t effectively stand-alone, and we definitely need to be planning for user error and test failure in the strategy.
Overall, though, my rebuttal to the imperfect use argument is very similar to the discussion on safer sex vs. abstinence in pregnancy and STI prevention. Even though we know condoms are 98% effective against STI and unwanted pregnancy with perfect use but only 86% effective under normal use, we don’t require people to seek professional help and supervision for their use, because we understand that 86% protection is better than 0% protection. Ideally, if your condom fails, you’re getting post-exposure care, like PlanB or pregnancy and STI testing, because none of these things is a perfect measure on its own, but each layer adds to the safer sex equation. In a similar vein, harm reduction measures for drug use like naloxone programs don’t stop people from using drugs (and some people think that should be the goal), but they do help reduce overdose deaths, one of the most risky parts of using.
Rapid antigen tests, like condoms and naloxone programs, are a harm reduction strategy that allows people to make less-risky decisions with as much information as possible. It made sense to ask people to skip gathering for quite a while, but we’re social creatures, and it’s very, very hard for us to never gather. Realistically, even I’m not willing to do that forever. Long-term abstinence expectations will almost always fail, and we know from other versions of this story that when people don’t have the information they need to make a safe choice, they’ll often make a dangerous one. We need to empower people to make safer, informed choices. Mina and the study authors argue, and I agree, that a public health rapid testing strategy requires education campaigns to ensure correct usage within a minimized margin of error, but that’s super possible. Roll the condom on the banana, demonstrate the dental dam, offer naloxone training, show how to collect enough saliva for a spit test. We could do this. And while it wouldn’t mean zero Covid, it would probably mean we could have Christmas without worrying that we’re going to kill Grandma, and that’s a benchmark I’m extremely eager to reach.
Peto, Tim, and UK COVID-19 Lateral Flow Oversight Team. “COVID-19: Rapid Antigen Detection for SARS-CoV-2 by Lateral Flow Assay: A National Systematic Evaluation for Mass-Testing,” January 26, 2021. https://doi.org/10.1101/2021.01.13.21249563.
Harmon, Alexander, Celina Chang, Nol Salcedo, Brena Sena, Bobby Brooke Herrera, Irene Bosch, and Laura E. Holberger. “Validation of an At-Home Direct Antigen Rapid Test for COVID-19.” JAMA Network Open 4, no. 8 (August 27, 2021): e2126931. https://doi.org/10.1001/jamanetworkopen.2021.26931.
From Michael Mina, adapted from Peto et al. COVID-19: Rapid Antigen detection for SARS-CoV-2 by lateral flow assay: a national systematic evaluation for mass-testing.
Michael Mina. “Rapid Tests Work Very Well to Answer 🧵 AM I INFECTIOUS and a RISK TO OTHERS This Is THE Public Health ? We Care about I Made a BIG Chart of Rapid Tests - Overall Sensitivity vs Any PCR Pos - What FDA Judges - Sensitivity If Infectious (97%!) - What We Actually Care about 1/ Https://T.Co/Or0L2R7Y4D.” Tweet. @michaelmina_lab (blog), September 15, 2021.

